What is an antibody-drug-conjugate or ADC?
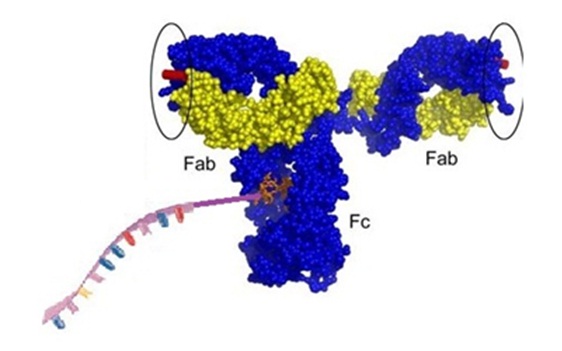
An ADC is an antibody molecule conjugated to a drug molecule via a linker group.
Antibody-drug conjugates, also called ADCs, are site-specifically modified antibodies that are designed as a targeted therapy for the treatment of cancer and are considered as a new class of highly selective, potent drugs. These complex molecules are made up of an antibody that is connected or conjugated to a cytotoxic drug via a stable chemical linker utilizing optimized coupling chemistries for their production. Sometimes a whole monoclonal antibody (mAb), a reengineered mAb or an antibody fragment, such as a single-chain variable fragment (scFv), is linked via a stable chemical linker with labile bonds, to a biological active drug.
Therefore, ADCs are pro-drugs with drugs covalently bound to monoclonal antibodies in which the antibody serves to deliver the drug to the intended site of action by binding to antigens at the site of action, for example to a tumor. To achieve this, the binding of the antibody has to be very specific to avoid off-target effects or binding. In addition the drug needs to be slowly released in the target cells. This type of drug is also called a toxophor and the total drug load has been called the “payload”. Since the total amount of conjugated drug or payload is limited, the toxophor has to exhibit a high potency. In addition, the drug to antibody ratio („DAR“) is critical for antibody stability.
However, to be useful as a therapeutic drug the pharmacokinetics, abbreviated as PK, of the ADC as well as the active drug has to be determined to evaluate efficacy, toxicity and the response to the drug exposure.
The use of biological therapies for the treatment of cancer is now a fast growing field. Unfortunately, the use of naked antibodies that show clinical efficacy has proven to be limited. To enhance the therapeutic potential of an antibody the conjugation to a small drug molecule has been heavily investigated in recent years. This approach is expected to combine the benefits of highly potent drugs with selective binders of specific tumor antigens. In addition, the next generation of ADCs are designed to utilize site-specific coupling chemistries using protein engineering with the aim to maintain the specificity and potency but to also improve the half-life, the homogeneity of drug loading, safety and quality of the therapeutic molecule. However, designing an ADC is a complex undertaking that requires the thoughtful combination of a selected antibody with a chemical linker group and a drug that targets a defined cancer indication. Lessons learned from the first-generation antibody-drug conjugates resulted in the improvement of the technology that now guides the design of new improved compounds, some of which are now in clinical trials. Intense research is ongoing to help improve ADCs further. Various linkers that show good in vitro stability and have a positive effect on ADC PK and in vivo efficacy are now designed and investigated.
As of 2013 a total of 27 ADC were undergoing clinical trials in both hematological malignancies and solid tumor indications. One ADC called T-DM1 or trastuzumab emtansine showed very promising results in phase III for the treatment of HER2-positive refractory/relapsed metastatic breast cancer. Other compounds currently in clinical trials are CMC-544, SAR3419, CDX-011, PSMA-ADC, BT-062, and IMGN901, targeting varied antigens. In additions, a search performed in April 2014 at “ClinicalTrials.gov” for the term “antibody-drug-conjugates” showed that 213 clinical trials were ongoing and some of them are recruiting.
Since the ADCs are exposed to different conditions during their journey from the blood vessels to the molecular target in the tumor tissue the mode of action of these drugs at the cellular or molecular level is complex. During circulation in the plasma the ADC must behave like a natural antibody and the linker must be stable. During antigen binding it is necessary that the conjugated antibody retains high immunoaffinity and the attached drug compound must not disturb this. During internalization a sufficient intracellular concentration of the drug must be achieved. After internalization during drug release the ADC has to efficiently release the original cytotoxic drug in its active form in the tumor. And finally, the inherent potency of the released drug must be sufficient to kill the tumor cells. These criteria demand that the ADCs are properly designed to achieve optimal effects.
References
ADC Review: Laurent Ducry and Bernhard Stump; Antibody-Drug Conjugates: Linking Cytotoxic Payloads to Monoclonal Antibodies. Bioconjugate Chem. 2010, 21, 5–13. [PubMed]
Makingn hot ADC: Sassoon I, Blanc V.; Antibody-drug conjugate (ADC) clinical pipeline: a review. Methods Mol Biol. 2013;1045:1-27. doi: 10.1007/978-1-62703-541-5_1. [PubMed]